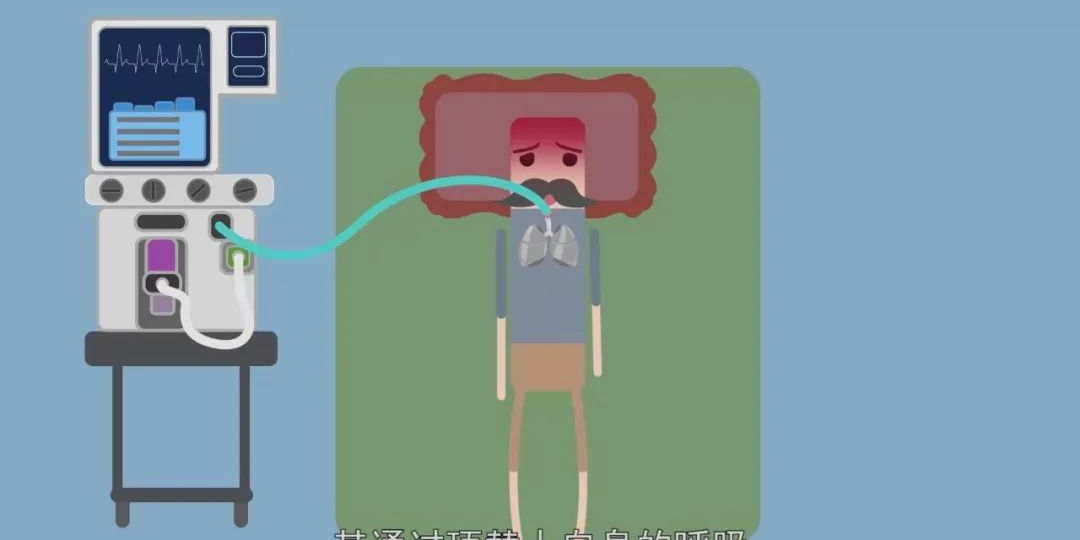
The anesthesia machine is one of the indispensable core devices in modern operating rooms. Its main function is to deliver anesthetic drugs to the patient's alveoli through a mechanical circuit during surgery, forming a partial pressure of anesthetic gas that diffuses into the blood and directly inhibits the central nervous system, thereby producing general anesthetic effects.
The anesthesia machine belongs to semi-open anesthesia devices. It mainly consists of an anesthesia vaporizer, flowmeter, folding bellows ventilator, breathing circuit (including inspiratory/expiratory unidirectional valves and manual breathing bag), corrugated tubing and other components.
With the continuous development of medical technology, the design of anesthesia machines has become increasingly intelligent and safe. So how exactly does an anesthesia machine work? What are its core principles and key components?

Air Anesthesia Machine
This device is lightweight and practical, directly using air and oxygen as carrier gases. It can provide assisted and controlled ventilation to meet various surgical requirements. Its working principle is: after completing anesthesia induction, connect the air anesthesia machine to a sealed mask or tracheal tube. During inhalation, the anesthetic gas mixture enters the patient's body through the open inspiratory valve; during exhalation, the expiratory valve opens while the inspiratory valve closes to expel exhaled gas. When using assisted or controlled ventilation, the folding bellows can be utilized - pressing down during inhalation and pulling up during exhalation to ensure adequate ventilation for the patient. Meanwhile, adjust the ether switch as needed to maintain stable anesthesia levels. The disadvantage of this device is its low ether concentration (only suitable for anesthesia maintenance), high ether consumption, and tendency to cause environmental pollution.
Direct Flow Anesthesia Machine
The direct flow anesthesia machine consists of high-pressure oxygen, pressure reducer, flowmeter, and anesthetic liquid vaporizer.
Circle Closed Anesthesia Machine
This device supplies patients with low-flow anesthetic gas mixture through unidirectional flow via a relief valve. Exhaled gas enters the CO2 absorber through the expiratory valve for reuse. Its structure mainly includes oxygen and nitrous oxide devices, gas flowmeters, vaporizer, CO2 absorber, unidirectional valves, breathing tubes, relief valve, reservoir bag, etc. Modern anesthesia machines are also equipped with ventilator airway pressure monitoring, expiratory flow monitoring, end-tidal CO2 concentration monitoring, inhaled anesthetic concentration monitoring, oxygen concentration monitors, hypoxia alarms and hypoxia-nitrous oxide automatic protection devices.
Structural Principle
Since Longning first applied ether anesthesia in 1846, inhalation anesthesia has become increasingly perfected. The development of modern pharmacology and technological advances, especially the application of computer technology, have greatly improved modern inhalation anesthesia. Inhalation anesthesia is easy to control, safe and effective, making it the preferred choice for hospital surgeries.
Anesthesia refers to methods that temporarily cause partial or complete loss of sensation in an organism to facilitate surgical treatment. There are various anesthesia methods such as acupuncture anesthesia, injection anesthesia and inhalation anesthesia. Hospitals mainly use inhalation anesthesia for general anesthesia. The anesthesia machine is the instrument that uses inhalation methods for general anesthesia.
Modern anesthesia machines are developing towards intelligent, integrated systems with coordinated, flexible and reliable component combinations, compact and reasonable structures, clear and user-friendly interfaces, and convenient operation. Electronically controlled gas delivery systems, built-in electronically controlled anesthesia ventilators, integrated breathing circuits, unified gas monitoring systems, and high/low microflow anesthesia methods represent the optimal combination of modern anesthesia machines. The new generation of anesthesia workstations will expand into the entire medical system, enabling networking with hospital equipment, defining and adjusting anesthesia processes and records, evaluating anesthesia effects, improving patient care quality, and creating a good working environment for clinicians. Modern anesthesia machines can be divided by structural principle into: gas supply and delivery system, anesthetic vaporizer, breathing circuit, anesthesia ventilator, safety monitoring system and waste gas scavenging system.
Gas Supply and Delivery System
The gas supply system includes: compressed gas cylinders (or central gas supply), check valves, overflow valves, filters, pressure gauges, gas pressure regulators, flowmeters, N2O-O2 ratio interlock control devices, and nitrous oxide-oxygen cutoff valves, etc.
Anesthesia machines must be equipped with flowmeters for various gas sources, with flowmeters in L/min and mL/min (or flow tubes below 2L/min) to facilitate low-flow anesthesia. They must also have N2O-O2 ratio interlock control devices to ensure the output anesthetic gas oxygen concentration is not less than 25%; when oxygen supply is insufficient or interrupted, nitrous oxide supply is automatically cut off. Common N2O-O2 ratio interlock control devices and nitrous oxide-oxygen cutoff valves are mechanical devices that must be carefully guarded against failure. During daily use, attention must be paid to the O2/N2O ratio, checking for flowmeter leaks, and relying on the anesthesia machine or other monitoring systems to measure O2 and N2O concentrations in the breathing circuit to more accurately assess current machine operation. Many modern anesthesia machines have a 55L/min oxygen bypass that can quickly and directly enter the breathing circuit through emergency interfaces, greatly facilitating anesthesiologists' oxygen delivery operations.
Anesthetic Vaporizer
The vaporizer (also called anesthesia evaporator or evaporation canister) is an important component of anesthesia machines. Its quality not only reflects the manufacturing level of the anesthesia machine but also directly affects the success of inhalation anesthesia and patient safety.
The basic principle of the vaporizer is to use changes in ambient temperature and heat sources to convert anesthetic drugs into vapor. A certain amount of carrier gas carries away saturated anesthetic gas to form an anesthetic vapor stream of certain concentration that directly enters the anesthesia circuit.
Breathing Circuit
The breathing circuit is the joint gas path device connecting the anesthesia machine to the patient, delivering anesthetic gas mixture to the patient and returning exhaled gas to achieve normal oxygen and carbon dioxide exchange. It mainly consists of breathing tubes, CO2 absorber, inspiratory/expiratory valves, reservoir bag, mask, machine control-manual control valve, exhaust valve, pressure limiting valve, open/semi-open valve, etc. Valves and tubes form directional gas circulation, using soda lime in the CO2 absorber to absorb CO2 and moisture to provide fresh gas to the patient. The machine control-manual control valve allows users to choose between manual control or machine control via the anesthesia ventilator; semi-open valves and pressure limiting valves enable flexible breathing circuit control and pressure limitation, facilitating spontaneous breathing.
Anesthesia Ventilator
The anesthesia ventilator has become an essential component of anesthesia machines. With the realization of mechanical ventilation in inhalation anesthesia, it has developed rapidly in recent years with comprehensive functions and miniaturization.
Anesthesia ventilator drives include pneumatic, pneumatic-electronic and electronic types. Pneumatic ventilators are older products that solely use compressed oxygen as the power source with high oxygen consumption, and are being phased out. Most newer anesthesia machine ventilators are oxygen-driven and electronically controlled. The latest anesthesia ventilators are built-in electronically controlled ventilators that don't require a drive gas and can use atmospheric air for ventilation in case of gas interruption to ensure patient safety. A typical anesthesia ventilator is a pneumatic-electronic ventilator where the inner and outer parts of the folding bag in the transparent sealed cover form two gas circuits - drive gas compresses the folding bag to deliver anesthetic gas to the patient, forming a dual-loop system of drive gas source and anesthetic gas flow.
Safety Monitoring System
Modern anesthesia machines all have safety monitoring systems. This system includes: oxygen supply deficiency alarm, oxygen deficiency/interruption nitrous oxide cutoff device, volume and concentration monitoring components and fault alarms. Monitoring components mainly include: inspired oxygen concentration, exhaled tidal volume, airway pressure, minute ventilation, end-tidal CO2 concentration, and anesthetic gas concentration. A microcomputer processes and displays various data with an attached alarm system, especially enabling respiratory, circulatory, neurological and muscular monitoring functions, greatly improving clinical anesthesia quality and patient safety, and increasing surgical success rates.
Waste Gas Scavenging System
The waste gas scavenging system collects excess residual gas from the anesthesia machine and exhaled waste gas from patients, then discharges it out of the operating room through pipes to avoid air pollution. It mainly includes waste gas collection and discharge devices consisting of: regulating valves, discharge valves, vacuum generators, pipes and connectors, etc.
Inhalation anesthesia delivers anesthetic drugs to the patient's alveoli through a mechanical circuit, forming a partial pressure of anesthetic gas that diffuses into the blood and directly inhibits the central nervous system to produce general anesthesia.
Air Anesthesia Machine
The air anesthesia machine is a semi-open anesthesia device. It mainly consists of a drug liquid canister, ether adjustment switch, folding bellows, inspiratory/expiratory unidirectional valves and corrugated tubes. As shown in Figure 2-1-1, this device is lightweight and practical, directly using air and oxygen as carrier gases to provide assisted and controlled ventilation for various surgical requirements.
Working Principle of Anesthesia Machines
The most common breathing circuit in anesthesia is the "circle system." Two unidirectional valves direct gas flow into a circular loop where CO2 is chemically absorbed. In this system, fresh gas from the anesthesia machine enters the breathing circuit downstream of the CO2 absorber and upstream of the inspiratory unidirectional valve. The incoming fresh gas mixes with existing gas in the circuit, flows through the inspiratory unidirectional valve, and passes through reusable or disposable corrugated tubing to reach the Y-piece. The patient's exhaled gas flows through the other branch of the circle system (expiratory limb), passing through the expiratory unidirectional valve into the reservoir bag. Squeezing the bag creates positive pressure, forcing collected gas through the CO2 absorber. Since fresh gas inflow exceeds what the patient and absorber consume, a relief valve must be installed between the expiratory unidirectional valve and CO2 absorber to vent excess gas when pressure exceeds set thresholds. The absorber canister contains soda lime (a mixture of sodium, potassium and calcium hydroxide) or baralyme (barium hydroxide octahydrate and calcium hydroxide). These substances chemically absorb CO2 while releasing heat and water (which humidifies the circulating gas). When absorption capacity is exhausted, an indicator changes color. The absorber design must facilitate absorbent replacement. The APL (adjustable pressure limiting) valve for venting excess gas is typically spring-loaded. Spring tension controls circuit pressure - during spontaneous breathing, the valve remains open allowing minimal resistance to airflow. For deeply anesthetized or paralyzed patients, the anesthetist may partially or fully close the valve to squeeze the reservoir bag and inflate the lungs for assisted/controlled ventilation. Waste gas from the APL valve should be scavenged outside the OR to avoid exposing staff to trace anesthetic gases.
After completing anesthesia induction, connect the air anesthesia machine to a sealed mask or tracheal tube. During inhalation, anesthetic gas mixture enters the patient through the open inspiratory valve; during exhalation, the expiratory valve opens while the inspiratory valve closes to expel exhaled gas. For assisted/controlled ventilation, use the folding bellows - compressing during inhalation and expanding during exhalation to ensure adequate ventilation. Adjust the ether switch as needed to maintain stable anesthesia levels. The disadvantages are low ether concentration (only suitable for maintenance), high ether consumption, and environmental pollution.
Direct Flow Anesthesia Machine
The direct flow anesthesia machine consists of high-pressure oxygen, pressure reducer, flowmeter and anesthetic liquid vaporizer. This device only provides oxygen and adjusts inhaled anesthetic concentration, requiring other devices connected in series at the output for anesthesia delivery.
Circle Closed Anesthesia Machine
This device supplies patients with low-flow anesthetic gas mixture through unidirectional flow via a relief valve. Exhaled gas enters the CO2 absorber through the expiratory valve for reuse. Its structure mainly includes oxygen and nitrous oxide devices, gas flowmeters, vaporizer, CO2 absorber, unidirectional valves, breathing tubes, relief valve, reservoir bag, etc. Modern anesthesia machines are also equipped with ventilator airway pressure monitoring, expiratory flow monitoring, end-tidal CO2 concentration monitoring, inhaled anesthetic concentration monitoring, oxygen concentration monitors, hypoxia alarms and hypoxia-nitrous oxide automatic protection devices. Before anesthesia, administer pure oxygen for 3-5 minutes, then proceed with anesthesia.
Components and Functions of Anesthesia Machines
Structurally, anesthesia machines consist of: frame, external circuit, anesthesia ventilator, anesthetic vaporizer, flowmeter, and monitoring system. Functionally, they comprise four main systems: gas supply and control circuit system, breathing and ventilation circuit system, scavenging system, and a set of system function and breathing circuit monitors. Some machines have additional monitors and alarms to indicate physiological variables and parameters related to cardiopulmonary function or gas/anesthetic concentrations in the breathing mixture. Manufacturers typically provide only basic monitoring and alarm configurations for standard models.
Below is an explanation of anesthesia machine composition and function based on working principles:
Circuit System
Since anesthesia machines require large oxygen volumes, they typically use hospital central supply systems or oxygen cylinders. Gases from cylinders pass through filters, check valves and regulators that reduce pressure to appropriate working levels (0.3-0.6 MPa). Central supply systems don't need regulators as pressure is already around 0.4 MPa. Most machines have oxygen failure alarms that reduce/cut other gas flows and trigger alarms if oxygen pressure falls below 0.28 MPa.
In continuous flow devices, each gas flow is controlled and displayed by flowmeters (mechanical or electronic LCD types). After passing control valves and flowmeters, gases enter the low-pressure circuit, passing through the vaporizer if needed before delivery to the patient. Proper machines have interlocked nitrous oxide-oxygen controls to prevent oxygen ratios below minimum (0.25 L/min).
Circle System
Most anesthesia machines provide continuous flow of oxygen and anesthetic gases in a circle system with two main breathing circuit types: closed and semi-closed. In closed circuits, all exhaled gas (after CO2 removal) returns to the system. Semi-closed circuits vent some exhaled gas. Low-flow anesthesia uses fresh gas flows below 1 L/min; minimal-flow below 0.5 L/min.
Manual ventilation requires squeezing the reservoir bag, which is tiring during long surgeries. Automatic ventilators mechanically deliver anesthetic gas mixture to the patient circuit while receiving exhaled and fresh gas. Anesthetists can adjust tidal volume, respiratory rate, I:E ratio and minute volume as needed.
Scavenging System
Also called CO2 absorption system, it contains 1-2 CO2 absorber canisters (filled with soda lime or baralyme) to remove CO2 from exhaled gas.
Monitoring and Alarm System
Anesthesia machines have various monitoring configurations for airway, physiological parameters, anesthetic gas concentrations, and indirect measures of anesthesia depth/muscle relaxation. Most include basic monitors for: airway pressure, inspired tidal volume, minute ventilation, respiratory rate and related alarms. Additional monitors can be added. Modern anesthesia workstations also incorporate anesthesia information management systems that collect, analyze and store clinical/administrative data, automatically generating anesthesia records.
As life-critical equipment ensuring anesthesia safety, anesthesia machines involve coordinated operation of multiple systems - from gas supply and anesthetic vaporization to breathing control and waste gas disposal - with each step impacting patient safety. Proper understanding of their principles helps medical staff operate them correctly and assists purchasers/managers in equipment selection.
For more information on models, specifications or procurement advice, please visit our product page or contact our technical consultants for professional support.




