Medical waste management is a critical and complex component of public health infrastructure and environmental protection. Generated in vast quantities daily by hospitals, clinics, laboratories, research facilities, veterinary practices, and even home healthcare, this waste stream poses unique risks due to its potential infectiousness, toxicity, and sheer volume. Among the various disposal methods employed globally—including autoclaving, chemical disinfection, microwaving, and landfilling—incineration remains a cornerstone technology, particularly for specific waste streams. Its effectiveness in neutralizing hazards, reducing volume, and enabling resource recovery offers distinct advantages. This article provides a comprehensive analysis of the multifaceted benefits of medical waste incineration, examining its technical, environmental, economic, and public health merits, while also acknowledging its limitations and the technological advancements mitigating them.

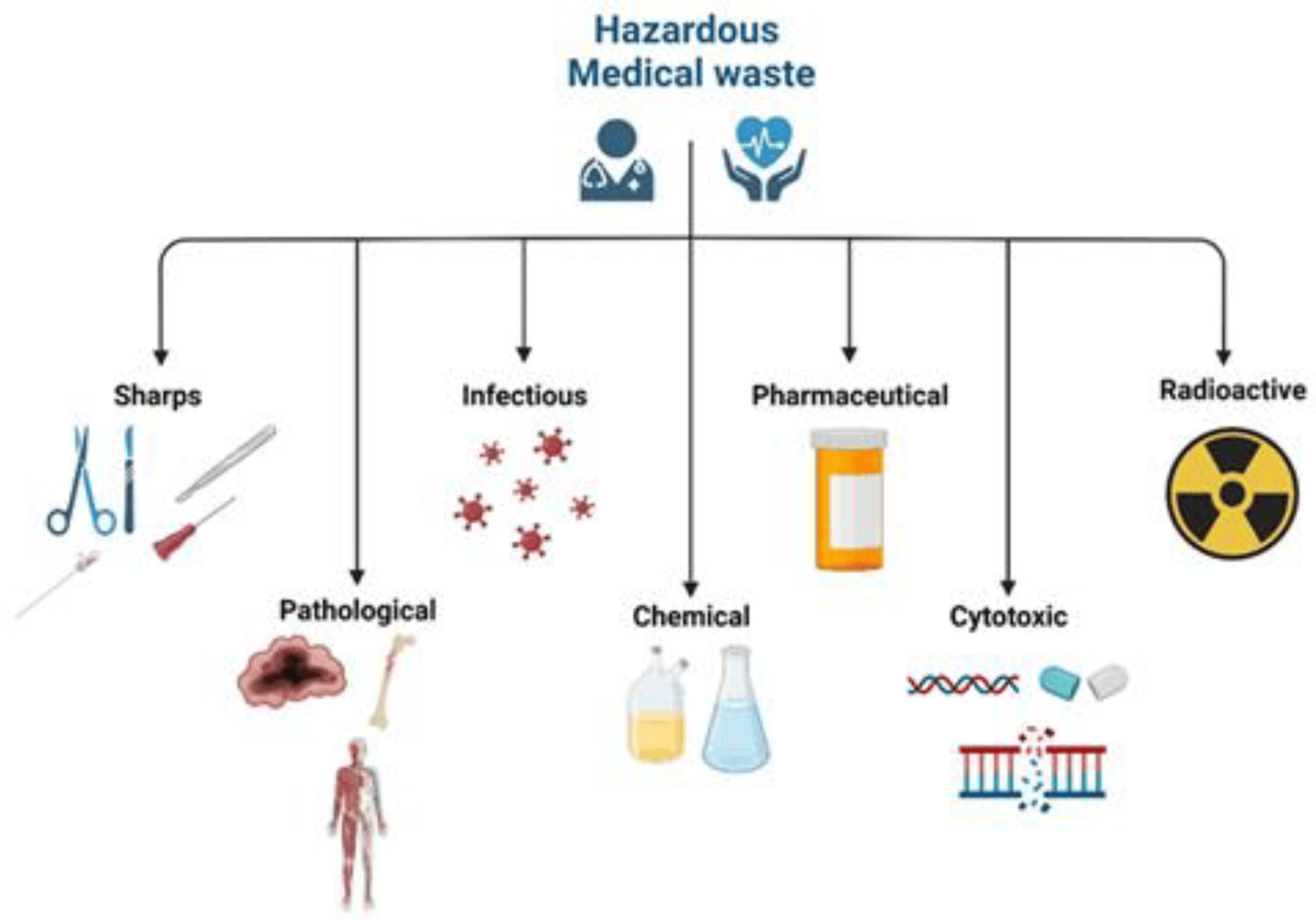
Medical waste, often termed healthcare waste (HCW), encompasses a highly heterogeneous mix of materials generated during diagnosis, treatment, immunization, or research involving humans or animals. Key categories include:
-
Infectious Waste: Materials contaminated with blood, bodily fluids, excreta, or pathogens (e.g., cultures, swabs, bandages, sharps like needles and scalpels).
-
Pathological Waste: Human tissues, organs, body parts, fetuses, blood, and fluids.
-
Sharps Waste: Needles, syringes, lancets, scalpels, broken glass.
-
Chemical Waste: Solvents, disinfectants, heavy metals (e.g., mercury from thermometers), batteries, photographic chemicals.
-
Pharmaceutical Waste: Expired, unused, spilt, or contaminated drugs, vaccines, sera.
-
Genotoxic Waste: Cytotoxic drugs used in cancer therapy, genotoxic chemicals.
-
Radioactive Waste: Unused liquids from radiotherapy or lab research, contaminated glassware, excreta from patients treated with radionuclides.
-
General/Household Waste: Non-hazardous waste not in contact with infectious materials.
The sheer diversity and hazard potential make safe disposal paramount. Improper management can lead to:
-
Disease Transmission: Sharps injuries expose waste handlers and the public to bloodborne pathogens (HIV, Hepatitis B & C).
-
Environmental Contamination: Pathogens, heavy metals, and persistent organic pollutants (POPs) leaching into soil and groundwater from landfills, or released untreated.
-
Antimicrobial Resistance (AMR): Discharge of inadequately treated waste containing antibiotics and resistant bacteria fuels the AMR crisis.
-
Chemical Toxicity: Exposure to hazardous chemicals via air, water, or soil.
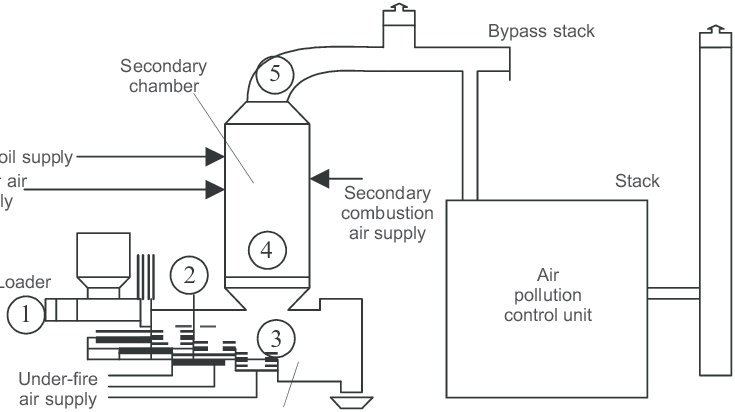
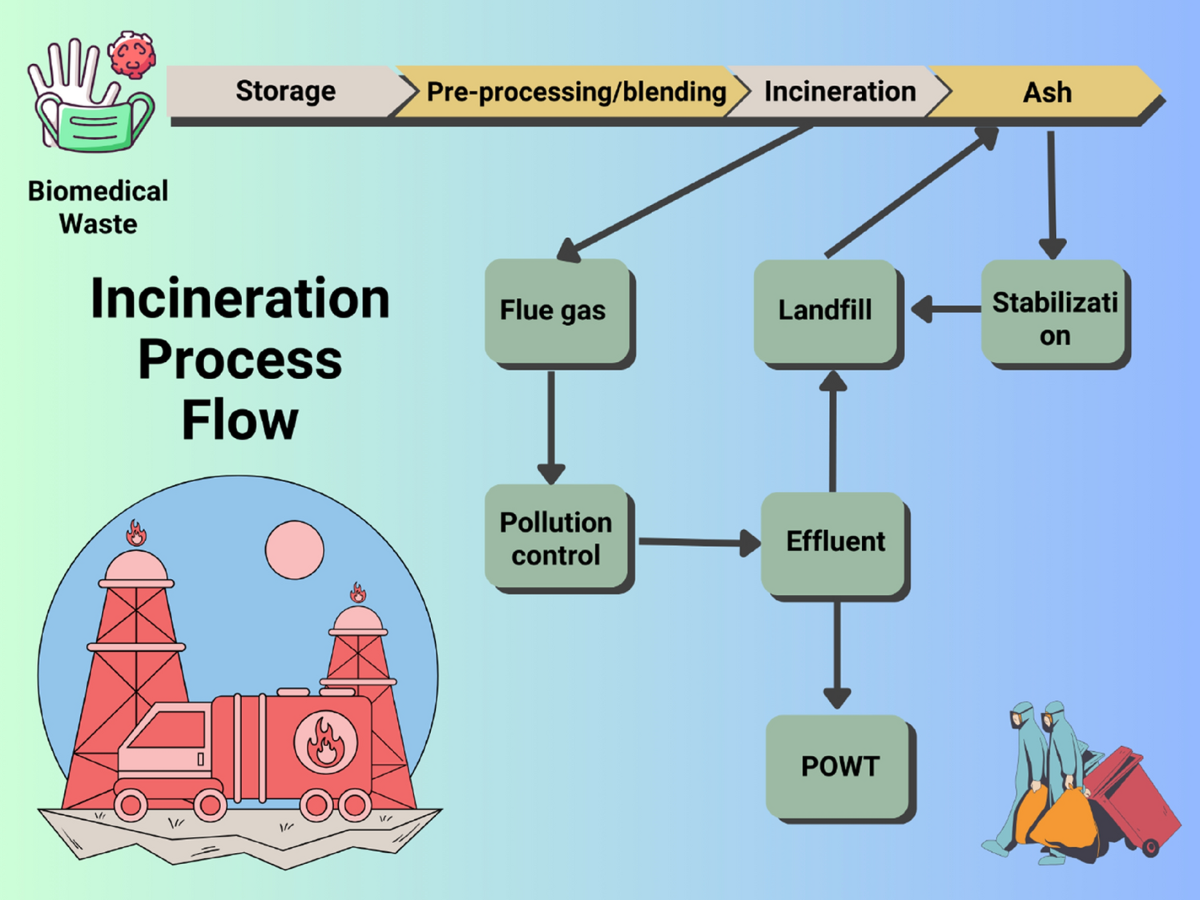
Incineration addresses these risks directly by subjecting waste to controlled, high-temperature combustion. The process involves feeding waste into a primary combustion chamber (typically operating between 800°C and 1000°C), where volatile components are vaporized and combusted. The resulting gases then pass into a secondary combustion chamber (often exceeding 1000°C, frequently mandated at >1100°C with 2+ seconds residence time) to ensure complete destruction of organic compounds, including complex hydrocarbons and dioxin precursors. The residual ash is collected, and the hot flue gases pass through sophisticated air pollution control (APC) systems before being released via a stack. Modern facilities convert the intense heat generated into usable energy (steam, electricity), embodying the waste-to-energy (WtE) principle.
2. Unparalleled Volume Reduction and Space Efficiency
This remains one of incineration's most tangible and critical advantages. Healthcare facilities, especially large hospitals in densely populated urban areas, generate enormous volumes of waste daily. Storage space is often limited and expensive, and transportation costs are directly proportional to volume and weight.
-
Mechanism: Incineration oxidizes the organic carbon and hydrogen content of waste, converting it primarily into carbon dioxide, water vapor, and inert inorganic ash. Plastics, a significant component of medical waste (syringes, IV bags, packaging), are particularly reduced as their polymer chains are broken down.
-
Quantifiable Impact: As the original article states, incineration achieves volume reductions of 90-95% and weight reductions of 70-90%. To illustrate: 10 tonnes of medical waste entering an incinerator results in only 0.5 to 1 tonne of ash requiring final disposal. Compare this to autoclaving, which sterilizes waste but leaves its physical form largely intact (reducing volume only through compaction, typically 60-70% at best), or landfilling, which offers zero reduction initially and relies on slow, incomplete biodegradation over decades.
-
Significance: This dramatic reduction has profound implications:
-
Reduced Landfill Burden: Minimizes the consumption of valuable and increasingly scarce landfill space. Landfills designed for hazardous waste (required for untreated medical waste in many jurisdictions) are particularly expensive to construct and maintain.
-
Lower Transportation Costs & Emissions: Fewer truckloads are needed to transport the residual ash compared to the original waste volume, reducing fuel consumption, traffic congestion, and associated greenhouse gas (GHG) emissions.
-
On-site Efficiency: For hospitals with small-scale incinerators (subject to strict regulations), significant volume reduction occurs on-site, easing storage and handling logistics before final ash disposal.
Table 1: Enhanced Waste Volume Reduction Comparison
| Disposal Method |
Volume Reduction (%) |
Weight Reduction (%) |
Residual Form |
Landfill Space Required |
Transport Needs |
| Incineration |
90 - 95% |
70 - 90% |
Inert Ash (3-5% of input) |
Very Low |
Very Low |
| Autoclaving/Sterilization |
60 - 70% (with compaction) |
Minimal (unless shredded) |
Sterilized, intact waste (often shredded) |
High |
High |
| Chemical/Microwave |
Minimal |
Minimal |
Treated, intact waste (often shredded) |
High |
High |
| Landfilling (Untreated) |
0% (initial) |
0% (initial) |
Original waste, decomposes slowly |
Very High |
Very High |
| Landfilling (Treated) |
Depends on treatment |
Depends on treatment |
Treated waste, still bulky |
High |
High |
3. Definitive Pathogen Destruction and Hazardous Substance Elimination
The core function of medical waste treatment is rendering it safe. Incineration excels in this domain due to the application of intense, controlled heat.
-
Pathogen Inactivation: Microorganisms (bacteria, viruses, fungi, spores, prions) are highly susceptible to thermal destruction. Modern medical waste incinerators operate at temperatures far exceeding the thermal death points of even the most heat-resistant pathogens (e.g., Bacillus stearothermophilus spores, used as biological indicators for autoclaves, are destroyed at 121°C in 15-30 minutes under steam pressure; incinerators operate continuously at 800-1100°C+). The high temperature, combined with sufficient residence time in the secondary chamber (ensuring all gases reach the required temperature for >2 seconds), guarantees near-total destruction (log 6 reduction or better) of all known pathogens, including resilient ones like Hepatitis B, HIV, Mycobacterium tuberculosis, and even prions associated with diseases like CJD, given optimal conditions. This level of certainty is crucial for pathological waste, sharps, and highly infectious materials.
-
Chemical Hazard Neutralization:
-
Pharmaceuticals: Incineration breaks down complex organic molecules found in drugs (including cytotoxics and antibiotics), preventing their entry into waterways where they can disrupt ecosystems and contribute to AMR. Modern high-temperature combustion effectively mineralizes these compounds.
-
Chemical Waste: Solvents, disinfectants, and reagents are oxidized into simpler, less harmful compounds (primarily CO2, H2O, inorganic acids captured in APC systems). Heavy metals present a different challenge (see Limitations & Ash Management).
-
Genotoxic Waste: Cytotoxic drugs are destroyed, preventing occupational and environmental exposure risks.
-
Sharps Neutralization: Needles and blades are melted and incorporated into the slag or ash, rendering them completely non-sharp and non-retrievable, eliminating injury risks post-treatment.
4. Energy Recovery and Contribution to Sustainability (Waste-to-Energy - WtE)
Modern medical waste incineration is not merely destruction; it's resource recovery. The substantial heat energy released during combustion is a valuable resource.
-
Energy Recovery Systems: Most large-scale and many modern hospital-scale incinerators incorporate sophisticated boiler systems. The hot flue gases pass through these boilers, transferring heat to water to produce:
-
Steam: Used directly for heating hospital buildings, sterilization (autoclaves), laundry facilities, or industrial processes.
-
Electricity: Steam drives turbines to generate electricity. This can power the incineration facility itself (significantly reducing operating costs) and feed surplus electricity into the local grid.
-
Quantifying the Benefit: The energy content of medical waste, particularly plastics and paper/cardboard, is significant, often comparable to low-grade coal ("Refuse Derived Fuel" - RDF). The recoverable energy depends heavily on the waste composition (plastics content) and plant efficiency.
-
Sustainability Contributions:
-
Fossil Fuel Displacement: Each unit of energy recovered from waste offsets the need to generate that energy from fossil fuels (coal, oil, natural gas), directly reducing CO2 emissions associated with energy production. *Note: While incineration releases CO2 from fossil-derived plastics, displacing fossil fuel generation usually results in a net GHG benefit.*
-
Resource Efficiency: Embodies the principle of recovering value from waste streams.
-
Reduced Reliance on Landfills: Landfills generate methane (a potent GHG) from decomposing organic matter. Diverting waste to WtE reduces landfill methane emissions.
| Facility Type & Scale |
Typical Waste Capacity (TPD*) |
Typical Energy Output |
Primary Use of Energy |
GHG Reduction Potential (vs. Landfill + Grid) |
Notes |
| Small-scale Hospital Unit |
0.1 - 1 TPD |
0.2 - 2 MW thermal |
On-site steam (heating, sterilization) |
Moderate |
Primarily reduces facility energy bills & fossil fuel use for steam. |
| Medium-scale Regional Plant |
5 - 15 TPD |
2 - 10 MW thermal / 0.5 - 3 MWe |
Steam for district heating / Electricity for grid |
Significant |
Balances waste disposal needs with local energy demand. |
| Large-scale Dedicated MWI |
20 - 100+ TPD |
10 - 50+ MW thermal / 3 - 20+ MWe |
Primarily electricity for grid, potentially steam cogeneration |
Very Significant |
High efficiency, major contributor to regional waste strategy & grid. |
| Co-incineration in WtE |
Varies (MW as % of MSW) |
Integrated into total plant output |
Electricity/Steam for grid/industry |
Significant (depends on mix) |
Utilizes spare capacity; strict emission controls still required. |
*TPD = Tonnes Per Day; MW = Megawatt (thermal or electrical); MWe = Megawatts electrical
5. Mitigating Broader Environmental Impacts: Beyond Emissions
While emissions are the most discussed environmental aspect, incineration's overall environmental profile, when done correctly, offers advantages compared to alternatives:
-
Advanced Air Pollution Control (APC): Modern incinerators are equipped with multi-stage APC systems that dramatically reduce emissions below stringent regulatory limits. These typically include:
-
Dry/Semi-Dry Scrubbers: Inject reagents (lime, activated carbon) to neutralize acids (HCl, SO2) and adsorb heavy metals and dioxins/furans.
-
Fabric Filters (Baghouses): Remove particulate matter (PM), including fine PM (PM2.5) and the particulates carrying adsorbed pollutants like heavy metals and dioxins. Efficiency >99.9%.
-
Selective Catalytic Reduction (SCR): Reduces nitrogen oxides (NOx) using a catalyst and ammonia injection.
-
Continuous Emission Monitoring Systems (CEMS): Provide real-time data on key pollutants (CO, O2, NOx, SO2, HCl, PM, often Hg) ensuring compliance and triggering corrective actions.
-
Dioxin/Furan Control: Formation of these persistent organic pollutants (POPs) is minimized by:
-
Combustion Optimization: High secondary chamber temperature (>850°C, often >1000°C), sufficient oxygen, turbulence, and residence time (>2 sec) ensure "complete combustion," destroying precursors.
-
Rapid Quenching: Quickly cooling flue gases through the boiler and scrubbers avoids the temperature window (250-400°C) where dioxins can re-form.
-
Activated Carbon Injection: Adsorbs any dioxins/furans that form.
-
Groundwater Protection: By diverting waste from landfills (especially untreated infectious or chemical waste), incineration significantly reduces the long-term risk of leachate formation and groundwater contamination. Even treated waste in landfills produces leachate requiring management.
-
Odor and Vector Control: Incineration completely destroys organic matter that attracts pests (flies, rodents) and causes putrefaction odors, issues often associated with waste storage and landfills.
-
Lifecycle Analysis (LCA): Comprehensive LCAs comparing incineration (with energy recovery) to other options like landfilling (even with pretreatment) often show incineration has a lower overall environmental footprint for non-recyclable hazardous waste streams, particularly concerning climate change (GHG), acidification, and eutrophication potential, when state-of-the-art APC is used.
6. Regulatory Compliance and Evolving Standards: Ensuring Safety
The safe operation of medical waste incinerators hinges on rigorous regulation and oversight. Standards have evolved significantly over decades, driven by environmental and health concerns.
-
Key Regulatory Frameworks:
-
USA: EPA regulations under the Clean Air Act (CAA), specifically Standards of Performance for New Stationary Sources (NSPS) and Emission Guidelines for Existing Sources (EG) for Hospital/Medical/Infectious Waste Incinerators (HMIWI). These set strict limits for PM, CO, HCl, SO2, NOx, Pb, Cd, Hg, dioxins/furans, and opacity. Requires CEMS, stack testing, operator training, and ash testing. RCRA governs ash disposal.
-
European Union: Strictly regulated under the Industrial Emissions Directive (IED - 2010/75/EU), incorporating Best Available Techniques (BAT) conclusions. BAT-AELs (Associated Emission Levels) set demanding limits for all major pollutants, including very low dioxin levels (0.1 ng TEQ/Nm³). Requires extensive monitoring and reporting.
-
International: The Stockholm Convention on Persistent Organic Pollutants (POPs) targets the minimization and ultimate elimination of dioxin/furan releases, directly impacting incinerator standards globally. WHO provides guidelines on safe HCW management.
-
Compliance Mechanisms: Modern facilities achieve compliance through:
-
Advanced Design: Optimized combustion chambers, high-efficiency APC systems.
-
Process Control: Sophisticated automation controlling feed rate, temperature, air supply.
-
CEMS: Continuous monitoring ensures real-time compliance and data recording.
-
Regular Testing: Periodic stack tests for pollutants not covered by CEMS (e.g., dioxins, metals).
-
Operator Training & Certification: Ensuring skilled personnel operate the complex systems.
-
Ash Characterization & Management: Treating ash as hazardous waste if necessary and disposing of it in secure landfills.
-
Transparency and Public Reporting: Regulatory compliance often includes public accessibility to emission data and permit conditions, fostering accountability.
7. Economic Considerations: Lifecycle Cost Analysis
Evaluating the economics of incineration requires a holistic, lifecycle perspective, moving beyond simple upfront costs:
-
Capital Costs: High. Constructing a modern, compliant incineration facility, especially a large-scale WtE plant, requires significant investment in specialized combustion technology, robust APC systems, energy recovery boilers/turbines, and sophisticated control systems.
-
Operating Costs: Moderate to High. Includes costs for:
-
Skilled labor (operators, technicians, maintenance)
-
Utilities (supplemental fuel during startup/shutdown, electricity for drives/fans)
-
Reagents (lime, activated carbon, urea for SCR)
-
Maintenance & Parts (high-temperature refractory, boiler tubes, APC components)
-
Ash disposal (transport and tipping fees at hazardous waste landfill if required)
-
Emission monitoring (CEMS operation, stack testing)
-
Regulatory compliance (permitting, reporting)
-
Revenue Streams / Cost Savings:
-
Waste Tip Fees: Facilities charge generators (hospitals, clinics) for accepting waste.
-
Energy Sales: Revenue from selling steam or electricity (major offset for large plants).
-
Avoided Costs: Savings from reduced landfill tipping fees (due to 90-95% volume reduction), reduced transportation costs (less waste/ash to move), potential savings from on-site steam use displacing purchased energy (for hospital units).
-
Long-Term Value & Cost-Effectiveness: While the initial investment and operating costs are substantial, the combination of waste disposal service revenue, energy sales revenue, and significant avoided costs (landfill, transport, fossil fuel purchase) makes modern, efficient WtE incineration a financially viable and often cost-competitive solution over its operational lifespan (20-30 years) for the appropriate waste streams and in contexts with high landfill costs or energy prices. It transforms a pure cost center (waste disposal) into a partial revenue generator.
Table 3: Detailed Comparative Cost Analysis (Lifecycle Perspective)
<td style="padding-top: 10px; padding-right: 10px; padding-bottom: 10px; border-bottom: 1px solid #e5e5e5; font-size: 15px; line-height: 1.72; border-top-color: #e5e5e5; border-right-color: #e5e5e5; border-left-color: #e5e5e5; min-width: 100px; max-width: max
| Disposal Method |
Capital Cost |
Operating Cost |
Revenue Potential |
Key Cost Drivers |
Key Cost Avoidance/Savings |
Long-Term Cost Effectiveness (Context Dependent) |
| Incineration (WtE) |
Very High |
Moderate-High |
Yes (Tip Fees, Energy) |
Plant construction, APC, maintenance, reagents |
Landfill fees (major), Transport, Fossil fuel |
Often High (Large scale, high landfill/energy costs) |
| Autoclaving/Sterilization |
Moderate |
Moderate |
Limited (Tip Fees only) |
Equipment, maintenance, labor, utilities |
Reduced infection risk cost |
Moderate |
| Chemical/Microwave |
Moderate |
Moderate-High |
Limited (Tip Fees only) |
Chemicals, equipment, maintenance, labor |
Reduced infection risk cost |
Moderate |






